
"Practicing" surgeon
What my violin taught me about being a resident

As a high school student, I was 100% going to become a professional violinist. I went to a boarding arts school, I was first-chair in the local youth symphony, and all of my friends were similarly obsessive young musicians. I even started college at a conservatory, before ultimately transferring to study nerdy science things at Columbia.
I don’t play much anymore, but all of my internal circuitry for learning was built and tested on 4 strings and some horsehair, and that’s never really gone away.
Throughout residency, I’ve puzzled over how becoming a surgeon is in many ways a similar challenge to becoming a violinist, but the two fields approach training in VERY different ways.
In music world, it’s “practice makes perfect.” In surgery world, it’s “see one, do one, teach one.” While both worlds have a heavy emphasis on reps (aka repetition) as the road to mastery, in music world you keep repping until you’re ready to go out there and perform. In surgery world, every rep is a performance.
I did a deep dive into the history of surgical training and the cognitive science of procedural learning to try to make sense of this. That research became an hour-long grand rounds talk, the juiciest bits of which I’ve highlighted below (and some I’ve already talked about on Insta).
I hope this sticks in your brain like it’s stuck in mine. Having a better “meta” understanding of what I’m doing has shaped how I approach residency, and helped me contextualize what’s wrong when things aren’t working.
Exceedingly brief history of why surgical training is the way it is
The Halsted Era (1880s-1930s): Dr. Halsted created the first surgical residency program. It was a Hunger Games vibe. Residents battled against one another for the attention of one man (Halsted himself) who decided when—if ever—they were ready to graduate. This was an inconsistent and unscalable system, but it is the primordial ooze from which our current system emerged.
The Churchill Model (1930s-1980s): Dr. Churchill turned this into something more structured and collegial. No more arbitrary rulings by your attending overlords: if you put in your time living (yes literally residing) in the hospital, you got to become a surgeon. This model started churning out a sustainable supply of surgeons with a moderately consistent skill set and knowledge base.
The ACGME Era (1980s-2010s): High-profile deaths linked to overworked, undertrained residents led to increased oversight by an alphabet soup of organizations. Graduating was still based on time-served, but now with much stricter rules, work hour limits, and standardized requirements.
Competency-Based Education (2010s-present): We are now in the midst of an evolution toward competency-based education: where measurements of performance increasingly guide the decision to graduate a resident, rather than time-served alone. We’re still in the early stages (particularly for plastics, which is a field where performance is extra-hard to measure), but this has the potential to make training better by focusing on the outcomes we actually care about, rather than time-served alone.
Ok I got the historical context, what about the science?
Learning to DO something is very different than learning information. If you’ve ever picked the wrong song at karaoke you know: just because you’ve listened to something a million times doesn’t mean it’s going to translate when you grab the mic.
Procedural learning in surgery, as in any field, requires a few key ingredients:
Working memory - This is the bottleneck of all learning, and an inherently limited resource. Your brain can only hold 7 plus or minus 2 active things at any one time. The problem is, doing surgery requires knowing more things than that. Additionally, your working memory capacity can be negatively affected by a wide variety of outside factors that are unfortunately inherent in surgical training: lack of sleep, distractions, stress, needing to pee, etc. And the only way that you can free up more spots in your working memory iiiiis….
Repetition - This is how stuff gets from your working memory into longterm storage, little by little freeing up space for more knowledge to make its way in through the working memory bottleneck. This is also essentially how we can justify the time-served model for surgical training: time-served is an approximate marker for number of reps.
Coaching - While common in other high performance fields from business to sports to aviation, coaching is still not a typical component of surgical training. We certainly do have mentorship, which covers some (but not all!) of what coaching means in other fields.
This is probably the area with the biggest potential for improving surgical training. One of the only randomized controlled trials I’ve seen in surgical education is about a coaching-based curriculum for a surgery rotation. Residents in the coaching model showed significant improvement in their operative skills. The residents in the traditional model showed no improvement at all.
Encoding - This is the active, on-purpose stuff that you do to try to help your brain store stuff better. Taking notes before and after cases. Reading. Reviewing. Asking questions. It’s hard and annoying but that’s just your brain reminding you that this stuff works.
The Three Stages of Skill Acquisition
Another useful way to think about this in surgery is through the classic Fitts and Posner model:
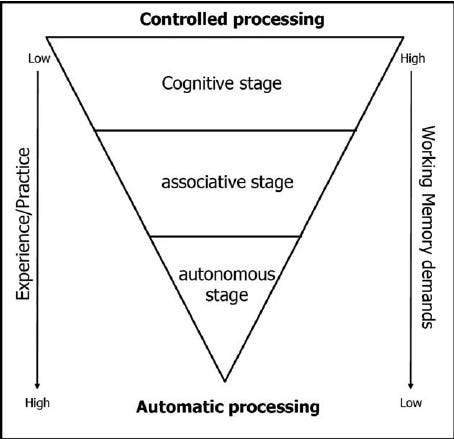
Cognitive Stage: Everything is new. You're relying on facts and conscious step-by-step thinking. Doing stuff is slow, you make mistakes, and it’s mentally exhausting. Think of medical-student-you using your whole brain to tie a knot.
Associative Stage: Steps start flowing together. You make fewer errors, your movements start to feel more fluid, but you’re still having to focus to get certain things right, and if you run into an unexpected problem, you feel totally lost. This is the intern who knows how to close an incision but sometimes their closure just looks bad and they can’t figure out why.
Autonomous Stage: True muscle memory. Your skill operates outside conscious awareness and does not require any working memory. You can close an incision automatically. You could probably do it in your sleep.
This progression requires reps over time. There's no shortcut. But again, that’s why time-served is not actually that terrible a proxy for surgical learning.
The irony of autonomy
Because the autonomous stage no longer involves any active recall, over time, you forget allllll of the facts and ideas that you used when you were first learning.
This is why learning from an attending can make you feel like an idiot: they are doing something that is simple for them, looks simple to you when you watch them do it, but in reality it’s a really complicated thing that they have forgotten the complexity of.
This phenomeneon leads to what’s called the “intermediate effect” in the psychology literature. Basically, the people best suited for teaching a task are often those who mastered it most recently. This is why trainee-to-trainee teaching is so powerful.
PennMicro: can we teach surgery like we teach music?
This meta-history-and-science rabbit hole led me to an experiment: working with one of my attendings (Dr. Suhail Kanchwala) who is also musical, we set out to see what it would look like to teach surgery like it’s music. We picked a discrete task that requires a distinct set of motor skills, and where opportunities for reps inside the OR are limited: sewing teeny-tiny blood vessels together (aka microvascular arterial anastomoses).
Like in music, we wanted to make reps “cheap,” aka something you could do easily anytime, anywhere with basic instruments (think: pens, paper, easily-liberated OR supplies). This also meant moving reps outside of the OR, and practicing for a few minutes every day, rather than in big, infrequent, multi-hour blocks as we typically do for surgical simulations.
We also wanted to break the complex process of sewing an anastomosis into a set of simple, discrete movements—sort of like scales or etudes in music—to allow trainees to focus in on building their muscle memory fundamentals.
We also incorporated coaching, since we have evidence that works: we had a few live practice sessions with trainees, and then we also had an ongoing text thread where we answered questions and assigned occasional “homework.”
The intermediate effect worked to my advantage: having recently learned these skills myself helped me bridge between my expert faculty attending (definitely in the autonomous phase) and our cognitive stage trainees.
This was just a small pilot project with a few trainees, but each of them was able to perform in the OR at a much higher level than is typical for their year of training. Trainees felt much better prepared for their first real microsurgery experiences, and that was reflected in faculty evaluations as well.
psst: if you want to see the videos yourself, they are all free online at www.pennmicro.org
Practicing surgeons
While the old dogs will talk your ears off back-in-my-daying about how easy we have it, the reality is that the way we train surgeons hasn't really changed that much in the last 100 years. Meanwhile, our health system has changed a LOT. Honestly, I'd say training now is probably more challenging because residents are expected to learn a larger, more complex set of skills with increased constraints on their time and autonomy.
The whole reason it's the "practice" of medicine is that it's not something you can just learn and then perform perfectly every time. You need reps. And just as in music, there's no number of reps that could ever make you perfect.
Small experiments like PennMicro show there's still room to grow. Time and resources will always be tight in medicine, and we have serious institutional inertia to contend with, but we owe it to our patients to keep making our training system better.
If you made it this far, thank you so much for reading!!! I have 299 subscribers to this monthly newsletter (free to sign up!) and I’m eager to keep growing - please share with a friend or two who you think might be into this particular brand of plastic surgery nerdiness.
I love this! I feel challenged and inspired to create more intentionality in the way I teach students. Many days it becomes “just jump in and I’ll talk you through it” which is definitely difficult for digesting! Thank you for sharing 💛
This is awesome! As a musician turned plastic surgery resident as well, I definitely miss the bite sized practice. I'll have to try this out